Peak 30-minute Cadence Indicator - An Appropriate Stepping Intensity Indicator in Free-living Environments
Abstract Body (Do not enter title and authors here): Introduction: Stepping activity (e.g., walking) is a convenient and dominant physical activity (PA) mode for the lay public. To date, no worldwide PA guidelines have included steps as a public health goal, potentially due to the inconclusive evidence on dose-response association of stepping intensity and health outcomes. Inconsistent stepping intensity indicators may explain the equivocal results. A comprehensive comparison of various stepping intensity indicators under a single large cohort is crucial for identifying the appropriate indicator.
Aims: Our study aimed to examine and compare the association of stepping intensity estimated by various peak-cadence indicators with all-cause (ACM), cardiovascular disease (CVD) and cancer mortality.
Methods: This prospective study included 70,174 UK adults wearing wrist-worn accelerometer. Stepping intensity was estimated by eight indicators (peak 1-, 5-, 10-, 15-, 20-, 25-, 30-, 60-min cadence: defined as the averaged steps/min of the highest but not necessarily consecutive mins). We assessed dose-response associations of stepping intensity with mortality outcomes using cox-restricted-cubic-spline model. We presented overlapping plots to visually compare the dose-response association among indicators on standardized cadence scale.
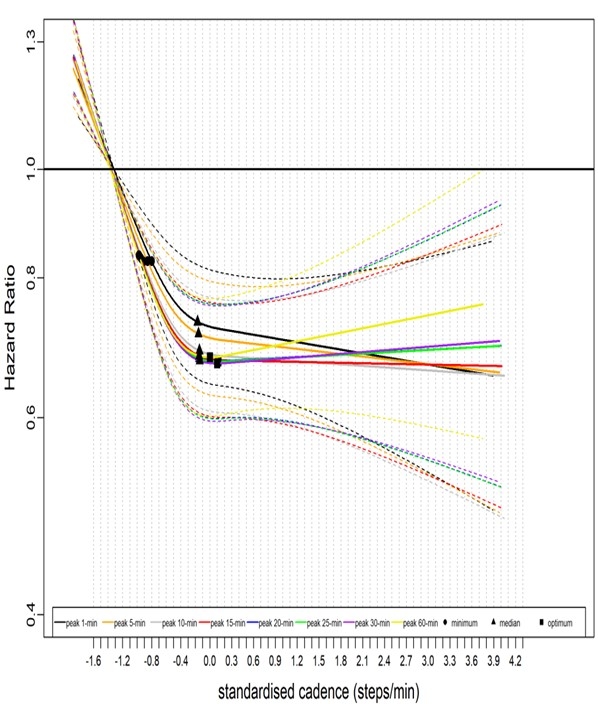
Results Longer peak time cadence provided a more pronounced inverse association with ACM/CVD mortality risk than shorter ones (i.e., peak 1-, 5-, 10- and 15-min cadence) at lower cadence scale (Fig.1,2). E.g., at -0.2 standardised steps/min, the ACM hazard ratio (HR) for peak 1-/30-min cadence were: 0.73, 95%CI (0.65, 0.82) and 0.65 (0.60, 0.70) (Fig.1). Peak 60-min cadence was associated with higher ACM/CVD mortality risk than other indicators at higher cadence scale, albeit with wide 95% CI. Higher stepping intensity was associated with lower cancer mortality in similar linear fashion across peak-cadence indicators, except for peak 60-min indicator. E.g., at 3.0 standardized cadence, the HR for peak 1-, 30-, and 60-min cadence were 0.76 (0.56, 1.01), 0.76 (0.56, 1.02) and 0.82 (0.59, 1.13) (Fig. 3).
Conclusions The longer peak time cadence indicators might be appropriate to reflect the association of lower stepping intensity with mortality risk. The scarcity of events at higher end of the scale precluded us from selecting specific peak-cadence indicator. Peak 30-min cadence provided the steepest association and is appropriate for representing stepping intensity in free-living setting.
Wei, Le
(
The University of Sydney
, Newtown , New South Wales , Australia )
Author Disclosures:
Le Wei:DO NOT have relevant financial relationships