Differences in Acute Myocardial Infarction and Heart Failure Cardiogenic Shock: Utilization of Temporary Mechanical Circulatory Support and Outcomes
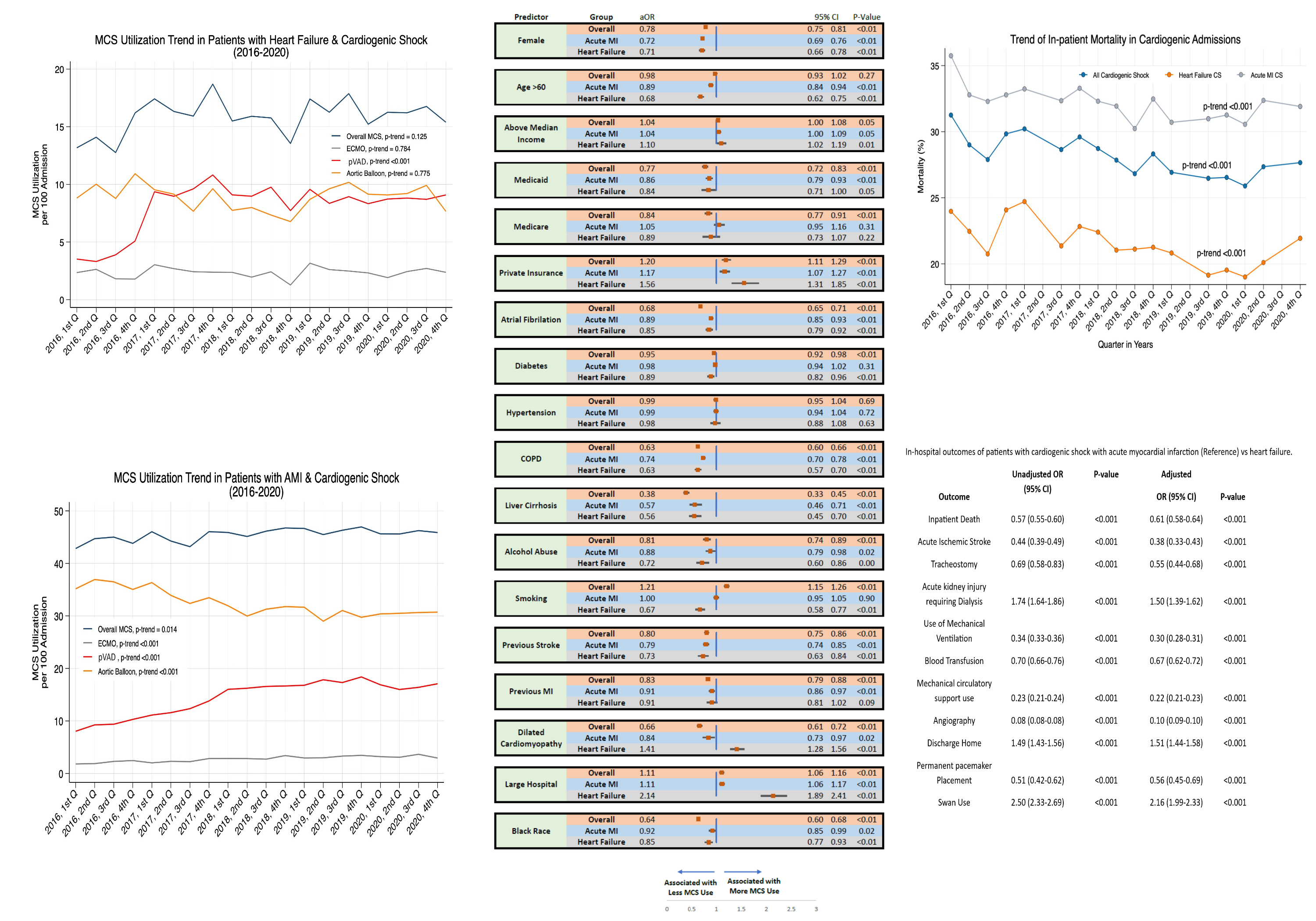
Abstract Body (Do not enter title and authors here): Introduction: Cardiogenic shock (CS) is marked by substantial morbidity and mortality. The two major CS etiologies include heart failure (HF) and acute myocardial infarction (AMI). The utilization trends of mechanical circulatory support (MCS) and their clinical outcomes are not well described. Methods: This study compares the rates of MCS utilization, factors associated with utilization, and clinical outcomes in patients who present with HF-CS and AMI-CS, using 2016-2020 National Inpatient Sample data. Results: The study included 329,280 patients, comprising 204,660 cases of AMI-CS and 124,620 of HF-CS. MCS utilization increased over the study period with variable degree among devices, and CS-phenotype. AMI-CS had higher intraaortic balloon pump (32.4% vs. 8.9%), extracorporeal membrane oxygenation (2.8% vs. 2.4%), and percutaneous ventricular assist device use (14.5% vs. 8.1%) compared to HF-CS (p<0.01). Factors linked to lower MCS use were female sex, age over 60 years, Black race, atrial fibrillation, chronic obstructive lung disease, diabetes mellitus, cirrhosis, previous stroke, or myocardial infarction. After adjusting for various factors, patients with HF-CS vs. AMI-CS had significantly fewer adverse outcomes, including inpatient death, stroke, tracheostomy, mechanical ventilation, and blood transfusion. However, HF-CS had higher odds of acute renal failure requiring dialysis. AMI-CS was associated with shorter hospital stays (8.8 vs. 15.0 days, p<0.001), lower charges ($251,580 vs. $294,792, p<0.001), and were less likely to discharge home. Conclusion: Despite the evolving trends in MCS utilization over time, CS patients still face high morbidity and mortality rates. The underlying shock etiology has a substantial impact on outcomes, with AMI cases demonstrating worse complications. This highlights the need for a personalized approach to CS management, considering not only etiology but also individual characteristics and comorbidities.
Alhuneafat, Laith
(
University of Minnesota
, Minneapolis , Minnesota , United States )
Ghanem, Fares
(
Southern Illinois University
, Detroit , Michigan , United States )
Jabri, Ahmad
(
Henry Ford Hospital
, Detroit , Michigan , United States )
Naser, Abdallah
(
Allegheny Health Network
, Pittsburgh , Pennsylvania , United States )
Bilal, Muhammad Ibraiz
(
Allegheny Health Network
, Pittsburgh , Pennsylvania , United States )
Al Akeel, Mohannad
(
East Tennessee State University
, Johnson City , Tennessee , United States )
Basir, Mir
(
Henry Ford Hospital
, Detroit , Michigan , United States )
Alexy, Tamas
(
University of Minnesota
, Minneapolis , Minnesota , United States )
Elliott, Andrea
(
University of Minnesota
, Minneapolis , Minnesota , United States )
Author Disclosures:
Laith Alhuneafat:DO NOT have relevant financial relationships
| Fares Ghanem:No Answer
| Ahmad Jabri:No Answer
| Abdallah Naser:No Answer
| Muhammad Ibraiz Bilal:DO NOT have relevant financial relationships
| Mohannad Al Akeel:DO NOT have relevant financial relationships
| Mir Basir:DO have relevant financial relationships
;
Consultant:Abiomed:Active (exists now)
; Consultant:Zoll:Active (exists now)
; Consultant:Saranas:Active (exists now)
; Consultant:Chiesi:Active (exists now)
; Consultant:Boston Scientific:Active (exists now)
| Tamas Alexy:DO have relevant financial relationships
;
Speaker:Abbott, Inc:Active (exists now)
; Research Funding (PI or named investigator):Endotronix:Active (exists now)
; Research Funding (PI or named investigator):Abbott, Inc:Active (exists now)
; Speaker:scPharmaceuticals:Active (exists now)
; Consultant:scPharmaceuticals:Active (exists now)
| Andrea Elliott:DO NOT have relevant financial relationships