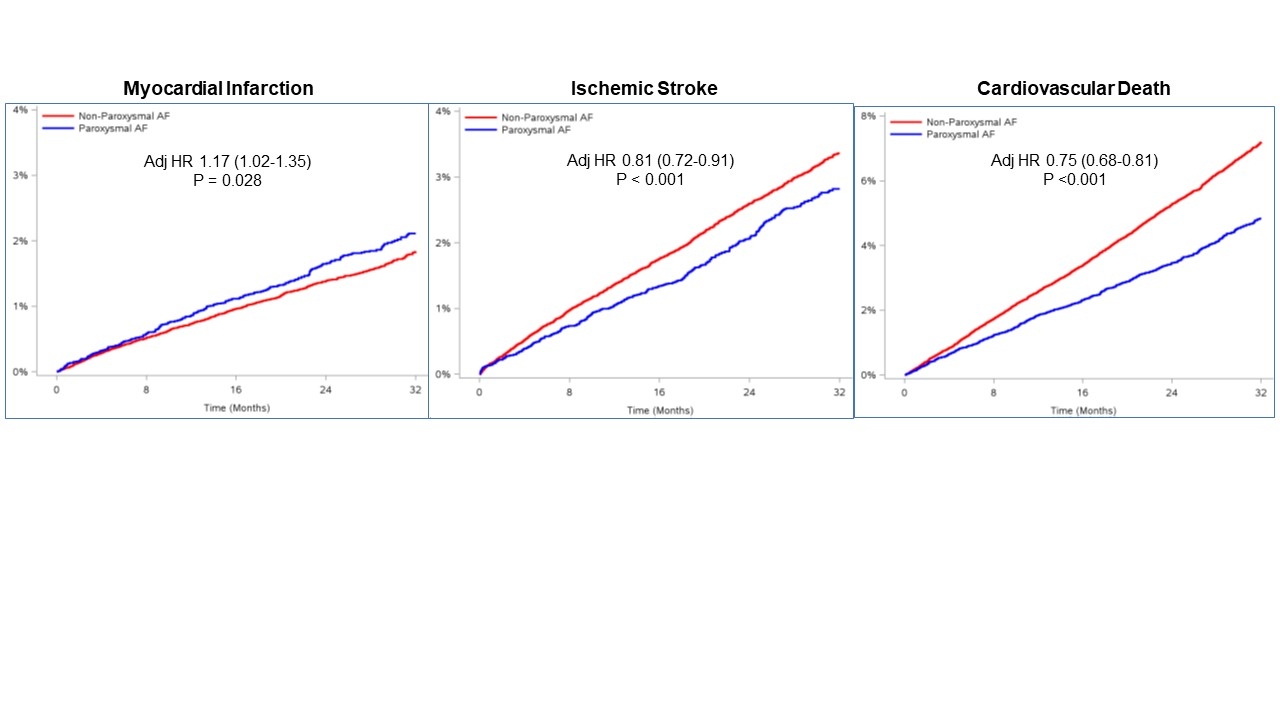
Risk of myocardial infarction in paroxysmal vs. non-paroxysmal atrial fibrillation: an individual patient-level data analysis of 71,466 patients from COMBINE AF
Abstract Body (Do not enter title and authors here): Background: Prior data suggest the MI risk may be higher with paroxysmal AF (PAF) vs. non-paroxysmal AF (non-PAF). Proposed mechanisms include tachycardia-induced oxidative stress (via LOX-1) with microvascular flow abnormalities, ischemia downstream of a fixed coronary obstruction, and plaque rupture. Methods: We compared MI rates in pts with PAF vs. non-PAF in COMBINE AF, a patient-level metanalysis of 4 RCTS of DOACs vs warfarin (ARISTOTLE, ENGAGE AF-TIMI 48, RE-LY,ROCKET AF). Secondary endpoints were ischemic stroke and CV death. Cox proportional-hazards models stratified by trial and adjusted for elements of the CHADS-VASc score were constructed. Sensitivity analyses were performed across subgroups, omitting pts on lower-dose DOAC regimens, and accounting for competing risk of death. Results: Of 71,466 pts, 16,609 (23%) had PAF at enrollment. Pts with PAF vs non-PAF were similar age (median 72 vs 72. P=0.15), but more likely women (43 vs 36%), with prior CAD (35 vs 31%), and on aspirin (41 vs 32%); but less likely Asian race (12 vs 15%) or with CHADS-VASc score > 4 (59 vs 60%), p<0.002 for each. During >160,000 pt-yrs of follow-up, 1033 MIs occurred: 277 (1.67%) in pts with PAF vs 766 (1.40%) in pts with non-PAF, corresponding to rates of 0.81% and 0.70% per pt-year. The HRadj for MI with PAF vs non--paroxysmal AF was 1.17 [1.02-1.35], p=0.028 (Fig). Ischemic stroke occurred in 364 (2.19%) vs 1425 (2.60%) pts with PAF vs non--paroxysmal AF (HRadj 0.81 [0.72-0.91], p<0.001). CV death occurred in 625 (3.77%) pts with PAF vs 3027 (5.52%) with non-paroxysmal AF (HRadj 0.75 [0.68-0.81], p<0.001). No significant effect modification of pt characteristics on MI risk by AF pattern were present, although a trend was seen for higher MI risk with PAF vs non-PAF in pts with prior CAD (HR 1.34 [1.12-1.59]) vs no prior CAD (HR 0.96 [0.76-1.22]), PINT 0.06. Results were consistent across trials, by anticoagulant, excluding lower dose DOACs, and accounting for competing mortality risk. Conclusions: This individual patient-level metanalysis of 71,466 pts from COMBINE AF shows that the adjusted risk of MI is higher in pts with PAF than non--paroxysmal AF, while the adjusted risks of ischemic stroke and CV death were lower in pts with PAF.
Ntaios, Georgios
(
University of Thessaly
, Katerini , Hawaii , United States )
Goette, Andreas
(
ST VINCENZ KRANKENHAUS
, Paderborn , Germany )
Palazzolo, Michael
(
TIMI Study Group
, Boston , Massachusetts , United States )
Antman, Elliott
(
BRIGHAM WOMENS HOSPITAL
, Boston , Massachusetts , United States )
Ruff, Christian
(
BRIGHAM WOMENS HOSPITAL
, Boston , Massachusetts , United States )
Braunwald, Eugene
(
TIMI Study Group
, Boston , Massachusetts , United States )
Link, Mark
(
UTSouthwestern Medical Center
, Dallas , Texas , United States )
Mahaffey, Kenneth
(
Stanford University
, Stanford , California , United States )
Eikelboom, John
(
McMaster University HGH
, Hamilton , Ontario , Canada )
Granger, Christopher
(
DUKE CLINICAL RESEARCH INSTITUTE
, Durham , North Carolina , United States )
Patel, Manesh
(
DUKE MEDICAL CENTER
, Durham , North Carolina , United States )
Wallentin, Lars
(
UPPSALA CLINICAL RESEARCH CENTRE
, Uppsala , Sweden )
Giugliano, Robert
(
TIMI Study Group
, Boston , Massachusetts , United States )
Author Disclosures:
Georgios Ntaios:No Answer
| Christopher Granger:DO have relevant financial relationships
;
Consultant:Alnylam:Active (exists now)
; Consultant:Pfizer:Active (exists now)
; Researcher:Boehringer Ingelheim:Past (completed)
; Consultant:Anthos:Active (exists now)
; Researcher:Anthos:Active (exists now)
; Consultant:Boston Scientific:Active (exists now)
; Researcher:Phillips:Active (exists now)
; Consultant:Janssen:Active (exists now)
; Researcher:Amgen:Active (exists now)
; Consultant:Merck:Active (exists now)
; Consultant:Novartis:Active (exists now)
; Consultant:Celecor:Active (exists now)
; Consultant:Roche:Active (exists now)
; Researcher:Roche:Active (exists now)
; Researcher:Alnylam:Active (exists now)
| Manesh Patel:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Bayer:Expected (by end of conference)
; Consultant:Esperion:Past (completed)
; Consultant:Bayer:Active (exists now)
; Research Funding (PI or named investigator):Idorsia:Active (exists now)
; Research Funding (PI or named investigator):Novartis:Active (exists now)
| Lars Wallentin:DO NOT have relevant financial relationships
| Robert Giugliano:No Answer
| Andreas Goette:DO NOT have relevant financial relationships
| Michael Palazzolo:No Answer
| Elliott Antman:DO have relevant financial relationships
;
Researcher:Itamar MEdical:Past (completed)
; Employee:AHA:Active (exists now)
| Christian Ruff:No Answer
| Eugene Braunwald:No Answer
| Mark Link:DO NOT have relevant financial relationships
| Kenneth Mahaffey:DO have relevant financial relationships
;
Research Funding (PI or named investigator):AHA:Active (exists now)
; Research Funding (PI or named investigator):Gilead:Past (completed)
; Consultant:Fuson:Active (exists now)
; Research Funding (PI or named investigator):Ferring:Past (completed)
; Consultant:Elsevier:Past (completed)
; Research Funding (PI or named investigator):Eidos:Active (exists now)
; Research Funding (PI or named investigator):CSL:Active (exists now)
; Consultant:CSL :Past (completed)
; Research Funding (PI or named investigator):California Institute Regenerative Medicine:Past (completed)
; Consultant:BridgeBio:Active (exists now)
; Consultant:BMS:Active (exists now)
; Consultant:Bayer:Active (exists now)
; Research Funding (PI or named investigator):Bayer:Active (exists now)
; Research Funding (PI or named investigator):Apple:Active (exists now)
; Consultant:Applied Therapuetics:Active (exists now)
| John Eikelboom:DO have relevant financial relationships
;
Consultant:Anthos:Active (exists now)
; Speaker:USV:Active (exists now)
; Speaker:Pfizer:Active (exists now)
; Speaker:Merck:Active (exists now)
; Speaker:Janssen:Active (exists now)
; Speaker:Ionis:Active (exists now)
; Speaker:Daiichi-Sankyo:Active (exists now)
; Speaker:BMS:Active (exists now)
; Speaker:BI:Active (exists now)
; Speaker:Bayer:Active (exists now)