Disparities in Healthcare Utilization following Endovascular Abdominal Aneurysm Repair
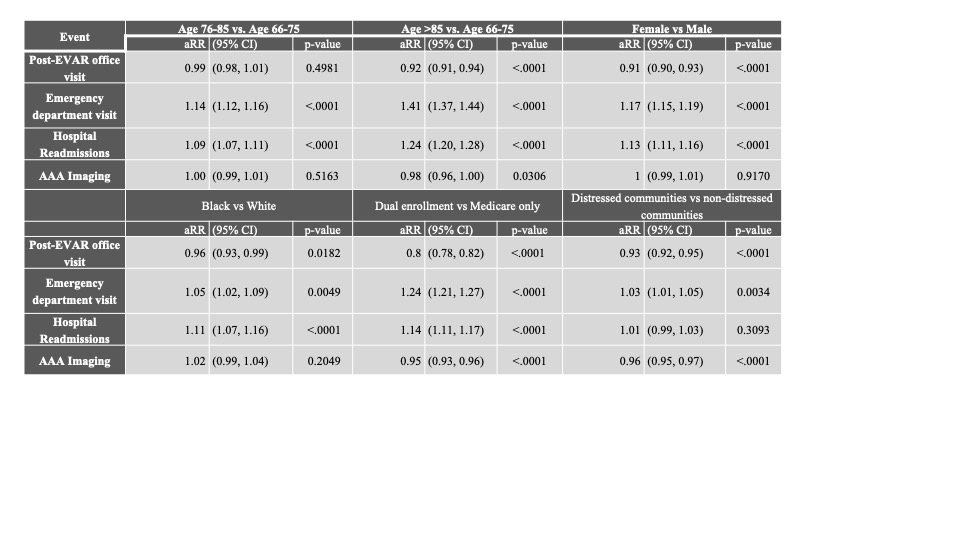
Abstract Body (Do not enter title and authors here): Introduction: Healthcare utilization in postoperative management and surveillance following endovascular aneurysm repair (EVAR) is an important factor in achieving long-term treatment success. However, factors associated with poor healthcare utilization have yet to be elucidated. Hypothesis: Disadvantaged patients have lower rates of surveillance and higher rates of emergency health service use than their counterparts. Aims: Examine rates of healthcare utilization stratified by age, sex, race, dual-enrollment in Medicare and Medicaid, and residence in a distressed community. Methods: We performed an observational retrospective cohort study of Medicare beneficiaries who underwent infrarenal EVAR with a bifurcated endograft between 2011-2019. We examined annual rates of post-operative surveillance (EVAR-related outpatient visits, surveillance imaging), use of emergency department (ED) visits, and hospital readmission across several disparity measures using Modified Poisson Regression models. Results: In 111,381 Medicare beneficiaries undergoing EVAR, comorbidities associated with poor postoperative surveillance were chronic kidney disease (aRR:1.06[1.04-1.07]), heart failure (1.10[1.09-1.11]), hyperlipidemia (1.16[1.14-1.19]), hypertension (1.09[1.07-1.12]), and ischemic heart disease (1.15[1.14-1.17]). For EVAR-related office visits, patients with worse post-operative care included those >85 years, female, Black, dual-enrolled, or living in distressed communities (Table 1). Similarly, less surveillance imaging was performed in patients >85 years, dual-enrolled, or living in distressed communities. There was a greater need for ER care or readmission among patients >85 years, female, Black, dual-enrolled, or living in distressed communities. Conclusions: Our study revealed patterns of disparities in post-procedure EVAR-related office visits and EVAR imaging studies, and greater use of emergency health services associated with patient age, sex, race, and socioeconomic status. These findings may suggest barriers in access to appropriate surveillance and care which could be addressed by targeting the identified groups for intervention efforts to improve EVAR surveillance.
St. John, Emily
(
BETH ISRAEL DEACONESS MED CENTER
, Boston , Massachusetts , United States )
Marcaccio, Christina
(
BETH ISRAEL DEACONESS MED CENTER
, Boston , Massachusetts , United States )
Ward, Rebecca
(
FDA
, Silver Spring , Maryland , United States )
Craig, Robert
(
FDA
, Silver Spring , Maryland , United States )
Gacchina Johnson, Carmen
(
FDA
, Silver Spring , Maryland , United States )
Torguson, Rebecca
(
FDA
, Silver Spring , Maryland , United States )
Fairman, Ronald
(
FDA
, Silver Spring , Maryland , United States )
Schermerhorn, Marc
(
BETH ISRAEL DEACONESS MED CENTER
, Boston , Massachusetts , United States )
Secemsky, Eric
(
BIDMC
, Boston , Massachusetts , United States )
Author Disclosures:
Emily St. John:DO NOT have relevant financial relationships
| Christina Marcaccio:No Answer
| Rebecca Ward:No Answer
| Robert Craig:DO NOT have relevant financial relationships
| Carmen Gacchina Johnson:DO NOT have relevant financial relationships
| Rebecca Torguson:DO NOT have relevant financial relationships
| Ronald Fairman:DO NOT have relevant financial relationships
| Marc Schermerhorn:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Medtronic:Active (exists now)
; Research Funding (PI or named investigator):Silk Road Medical:Active (exists now)
; Research Funding (PI or named investigator):Shape Memory:Active (exists now)
| Eric Secemsky:DO have relevant financial relationships
;
Consultant:Abbott/CSI, BD, BMS, Boston Scientific, Cagent, Conavi, Cook, Cordis, Endovascular Engineering, Gore, InfraRedx, Medtronic, Philips, RapidAI, Rampart, Shockwave, Terumo, Thrombolex, VentureMed, Zoll:Active (exists now)