Trends and Regional Variations in Chronic Ischemic Heart Disease and Lung Cancer-Related Mortality among American Adults: Insights from Retrospective CDC-Wonder Analysis
Abstract Body (Do not enter title and authors here): Introduction: Lung cancer remains the leading cause of malignancy-related mortality in the US. When concomitant Chronic Ischemic Heart Disease (CIHD) exists, morbidity and mortality in these patients is severely worsened. However, empirical evidence on shared mortality burden remains understudied. Therefore, we aim to retrospectively analyze mortality trends among American adults with concomitant lung cancer and CIHD.
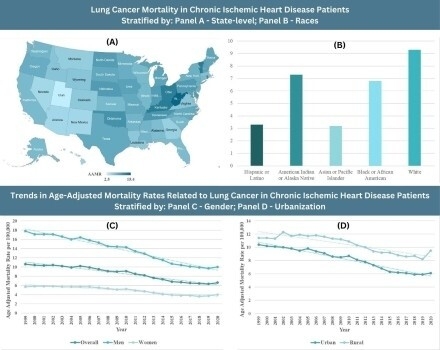
Methods: Death certificate data from the Centers for Disease Control and Prevention Wide-Ranging OnLine Data for Epidemiologic Research (CDC WONDER) database, using ICD-10 codes was retrieved for patients aged ≥ 45 years between 1999-2020. Age-adjusted mortality rates (AAMRs), per 100,000 people, and Annual Percentage Change (APCs) along with their respective 95% CIs were also calculated. Data was stratified according to year, sex, race, and geographical distribution.
Results: Lung cancer with comorbid CIHD in adults aged ≥ 45 years resulted in 214,785 deaths, with an overall AAMR 8.4 (95% CI: 8.3 to 8.4). The AAMRs remained relatively stable from 1999-2005 (APC: -0.8352; 95% CI: -1.9139 to 1.5413) succeeded by periods of significant decrease from 2005-2010 (APC: -2.3654; 95% CI: -5.5832 to -0.6062) and 2010-2017 (APC: -4.7159; 95% CI: -7.6110 to -3.6000). However, another period of stability was noted between 2017-2020 (APC: 0.8579; 95% CI: -2.1682 to 5.2231). In 1999, men had triple the mortality rate when compared with women (AAMR: 17.8 vs 5.7), which non-significantly declined in 2020 (AAMR:13.3 vs 4) respectively. Non-Hispanic (NH) Whites had highest AAMR (9.3), followed by NH American Indian or Alaskan Native (7.3), NH Black or African American (6.8), Hispanic or Latino (3.3) and lastly NH Asian or Pacific Islander (3.2). Furthermore, AAMRs also varied significantly in census regions, with the highest ratios being observed in the Midwest (9.6), followed by the Northeast (8.8), South (8.4) and lastly the West (6.8). Additionally, non-metropolitan areas were found to have comparably higher AAMRs than metropolitan areas (10.3 vs 8). States in the top 90th percentile such as West Virginia, Kentucky, Vermont, Ohio and Rhode Island had nearly triple the AAMRs when compared with states in the lower 10th percentile including Utah, Nevada, Arizona, New Mexico and Hawaii.
Conclusion: Mortality rates declined among American adults, with highest AAMRs being observed in men, NH Whites, residents of the Midwest and non-metropolitan patient populations.
Ali, Eman
(
Dow medical College
, Karachi , Pakistan )
Alim Ur Rahman, Hafsah
(
Dow medical College
, Karachi , Pakistan )
Salman, Madiha
(
Dow medical College
, Karachi , Pakistan )
Fahim, Muhammad Ahmed Ali
(
Dow medical College
, Karachi , Pakistan )
Shaikh, Asim
(
Dow medical College
, Karachi , Pakistan )
Ahmed, Jawad
(
Dow medical College
, Karachi , Pakistan )
Hameed, Ishaque
(
Medstar Health
, Baltimore , Maryland , United States )
Yasmin, Farah
(
Yale School of Medicine
, New Haven , Connecticut , United States )
Cheema, Huzaifa Ahmad
(
King Edward Medical University
, Lahore , Pakistan )
Ahmad, Adeel
(
Mass General Brigham-Salem Hospital
, Salem , Massachusetts , United States )
Author Disclosures:
Eman Ali:DO NOT have relevant financial relationships
| Adeel Ahmad:DO NOT have relevant financial relationships
| Hafsah Alim Ur Rahman:DO NOT have relevant financial relationships
| Madiha Salman:DO NOT have relevant financial relationships
| Muhammad Ahmed Ali Fahim:DO NOT have relevant financial relationships
| Asim Shaikh:DO NOT have relevant financial relationships
| jawad ahmed:DO NOT have relevant financial relationships
| Ishaque Hameed:DO NOT have relevant financial relationships
| Farah Yasmin:DO NOT have relevant financial relationships
| Huzaifa Ahmad Cheema:DO NOT have relevant financial relationships