Prognostic Characteristics of Patients with Electrocardiograms Masquerading as ST Elevation Myocardial Infarction
Abstract Body (Do not enter title and authors here): Background: Prehospital identification of STEMI reduces time to reperfusion by timely primary PCI or fibrinolytic therapy. We previously reported that 40-50% of prehospital ECG transmissions meeting Glasgow algorithm (GA) criteria for STEMI did not meet STEMI criteria on adjudication using the 4th Universal Definition of MI (4UDMI). These cases, herewith called ‘masquerading STEMI’, had high rates of late clinical complications. Here, we determined clinical factors predictive of late clinical outcomes among patients with masquerading STEMI.
Methods: From June 2010 to October 2021, 2,992 patients with prehospital ECG transmissions to Liverpool Hospital, Sydney, Australia, who met GA criteria for STEMI were identified. These were adjudicated according to the 4UDMI as confirmed STEMI or masquerading STEMI. Using multivariate logistic regression, we identified baseline patient characteristics that were associated with the outcome of cardiovascular death, MI and stroke at 2 years, among the masquerading STEMI cohort.
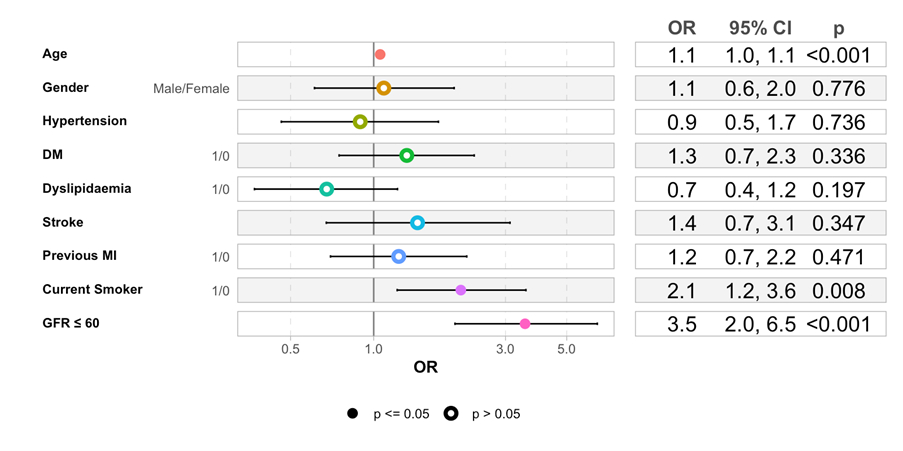
Results: 1553 (51%) patients were true-positive STEMI, while 1439 (49%) were masquerading STEMI. In the masquerading STEMI cohort, age, current smoking, and CKD (eGFR<60) were significant predictors of the 2-year cardiovascular death, MI stroke with OR of 1.05, 2.07, and 3.58, respectively (p<0.05 for all). Diabetes predicted MI re-presentation within 2 years (OR 3.76, p<0.05), and CKD predicted heart failure hospitalisation (OR 2.55, p<0.05).
Conclusions: Among patients with masquerading STEMI, current smoking and CKD were associated with the 2-year cardiovascular death, MI stroke. Diabetes predicted a higher risk of re-presenting with MI within 2 years, and CKD predicted a higher risk of hospitalisation with heart failure. Therefore, in this cohort of patients with masquerading STEMI, despite not having a true STEMI, smoking cessation and opportunistic management of diabetes and CKD may modify prognosis.
Fathieh, Sina
(
Kolling Institute
, Pymble , New South Wales , Australia )
Tran, Tu Hao
(
LIVERPOOL HOSPITAL
, Sydney , New South Wales , Australia )
Faour, Amir
(
Medcare Hospital
, Dubai , United Arab Emirates )
Dang, Viet
(
LIVERPOOL HOSPITAL
, Sydney , New South Wales , Australia )
Aljazaery, Asala
(
University of Sunderland
, Sunderland , United Kingdom )
Gibbs, Oliver
(
Liverpool Hospital
, Toongabbie , New South Wales , Australia )
Assad, Joseph
(
Liverpool Hospital
, Toongabbie , New South Wales , Australia )
Faddy, Steven
(
NSW Ambulance
, Sydney , New South Wales , Australia )
Long, Mitchell
(
University of New South Wales
, Sydney , New South Wales , Australia )
Pahn, Reece
(
LIVERPOOL HOSPITAL
, Sydney , New South Wales , Australia )
Rajaratnam, Rohan
(
LIVERPOOL HOSPITAL
, Sydney , New South Wales , Australia )
Lo, Sidney
(
LIVERPOOL HOSPITAL
, Sydney , New South Wales , Australia )
Juergens, Craig
(
Liverpool Hospital
, Liverpool , New South Wales , Australia )
Tam, Gladys
(
University of New South Wales
, Sydney , New South Wales , Australia )
French, John
(
LIVERPOOL HOSPITAL
, Sydney , New South Wales , Australia )
Author Disclosures:
Sina Fathieh:DO NOT have relevant financial relationships
| Reece Pahn:No Answer
| Rohan Rajaratnam:No Answer
| Sidney Lo:No Answer
| Craig Juergens:DO NOT have relevant financial relationships
| Gladys Tam:DO NOT have relevant financial relationships
| John French:DO NOT have relevant financial relationships
| Tu Hao Tran:No Answer
| Amir Faour:DO NOT have relevant financial relationships
| Viet Dang:No Answer
| Asala Aljazaery:DO NOT have relevant financial relationships
| Oliver Gibbs:No Answer
| Joseph Assad:DO NOT have relevant financial relationships
| Steven Faddy:DO NOT have relevant financial relationships
| Mitchell Long:No Answer