Clinical outcomes of cardiac synchronization with or without an implantable cardioverter defibrillator based on pooled data from 5 clinical trials: a patient-level meta-analysis
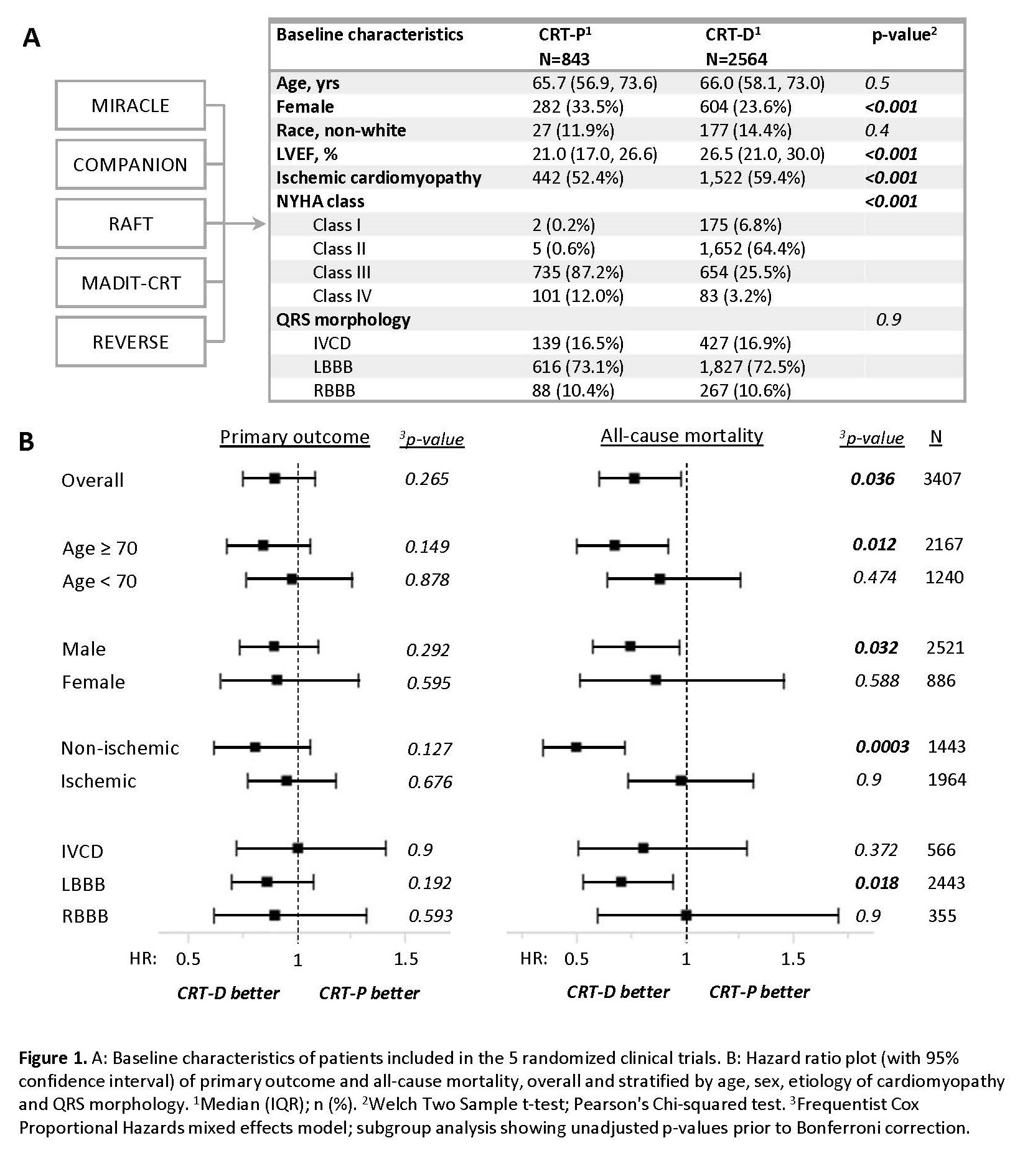
Abstract Body (Do not enter title and authors here): Background: Cardiac resynchronization therapy (CRT) is a well-established therapy for patients with heart failure with reduced ejection fraction (HFrEF) and wide QRS. Whether CRT-defibrillators (CRT-D) reduce mortality more than CRT-pacemakers (CRT-P) remains controversial. Aims: To compare the clinical outcomes of CRT-D vs CRT-P using data from 5 landmark CRT trials, both overall and stratified by etiology of cardiomyopathy (ischemic vs non-ischemic), sex (male vs female), age (≥ 70 y/o vs < 70 y/o), and QRS morphology (IVCD, LBBB, RBBB). Methods: We performed a meta-analysis of patient level data from 5 prospective CRT trials (MIRACLE, REVERSE, RAFT, COMPANION and MADIT-CRT). Inclusion criteria were CRT-P vs CRT-D status (randomized comparison only in COMPANION), age ≥ 18 y/o and LVEF ≤ 35%. Exclusion criteria included secondary prevention ICD, QRS < 120ms, pacemaker upgrade, ventricular pacing indication, or missing data. Primary outcome was composite of time to heart failure hospitalization (HFH) or all-cause death. Secondary outcomes were time to HFH and death. Outcomes were analyzed using a frequentist Cox Proportional Hazards mixed effects model adjusted for 17 variables. Results: A total of 3407 patients met inclusion criteria. Relative to patients with CRT-P (n=843), those with CRT-D (n=2564) were of similar age (66 y/o, p=0.5), less often female (24% vs 34%, p<0.001), and more often had ischemic cardiomyopathy (59.4% vs 52.4%, p<0.001), Fig 1A. Primary outcome was similar across groups (HR 0.902 [0.752, 1.081], p=0.26), but all-cause mortality was lower with CRT-D vs CRT-P (HR 0.77 [0.603, 0.983], p=0.036), Fig 1B. Interaction analyses suggested lower all-cause mortality with CRT-D vs CRT-P in patients with non-ischemic cardiomyopathy (HR 0.502 [0.346, 0.726], p=0.0003) and patients age ≥70 y/o (HR 0.679 [0.502, 0.919], p=0.012), with significance preserved after Bonferroni correction (Fig 1B). Conclusion: In patients receiving CRT for HFrEF, those with CRT-D had lower all-cause mortality than patients with CRT-P, driven mainly by a lower mortality with CRT-D in older patients and those with non-ischemic cardiomyopathy. No significant interactions were noted between ICD & sex or ICD & QRS morphology.
Shadrin, Ilya
(
DUKE UNIVERSITY MEDICAL CENTER
, Durham , North Carolina , United States )
Inoue, Lurdes
(
University of Washington
, Seattle , Washington , United States )
Schmidler, Gillian
(
Duke Clinical Research Institute
, Durham , North Carolina , United States )
Mackenzie, Michael
(
Duke Clinical Research Institute
, Durham , North Carolina , United States )
Friedman, Daniel
(
DUKE UNIVERSITY MEDICAL CENTER
, Durham , North Carolina , United States )
Abraham, William
(
Ohio State University
, Powell , Ohio , United States )
Cleland, John
(
University of Glasgow
, Glasgow , United Kingdom )
Curtis, Anne
(
University at Buffalo
, Buffalo , New York , United States )
Gold, Michael
(
MEDICAL UNIVERSITY SOUTH CAROLINA
, Charleston , South Carolina , United States )
Kutyifa, Valentina
(
UNIVERSITY OF ROCHESTER
, Rochester , New York , United States )
Linde, Cecilia
(
Karolinska Institutet
, Stockholm , Sweden )
Young, James
(
CLEVELAND CLINIC
, Chagrin Falls , Ohio , United States )
Tang, Anthony
(
Western University
, London , Ontario , Canada )
Al-khatib, Sana
(
DUKE UNIVERSITY MEDICAL CENTER
, Durham , North Carolina , United States )
Author Disclosures:
Ilya Shadrin:DO NOT have relevant financial relationships
| Valentina Kutyifa:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Boston Scientific:Past (completed)
; Speaker:Biotronik:Past (completed)
; Speaker:Abbott:Past (completed)
; Speaker:Medtronic:Past (completed)
; Research Funding (PI or named investigator):Zoll:Past (completed)
; Consultant:Biotronik:Active (exists now)
; Consultant:Zoll:Active (exists now)
; Research Funding (PI or named investigator):NIH:Active (exists now)
; Research Funding (PI or named investigator):Spire Inc:Active (exists now)
; Research Funding (PI or named investigator):Biotronik:Active (exists now)
| Cecilia Linde:DO have relevant financial relationships
;
Consultant:astra zeneca:Active (exists now)
; Research Funding (PI or named investigator):swedish academy of science:Active (exists now)
; Research Funding (PI or named investigator):swedish heart lungfoundation:Active (exists now)
; Advisor:medtronic:Active (exists now)
; Speaker:Impulse dynamics:Active (exists now)
; Speaker:boehringer ingelheim:Past (completed)
; Speaker:vifor:Past (completed)
; Speaker:medtronic:Active (exists now)
| James Young:DO NOT have relevant financial relationships
| Anthony TANG:DO NOT have relevant financial relationships
| Sana Al-Khatib:DO have relevant financial relationships
;
Other (please indicate in the box next to the company name):AHA:Active (exists now)
| Lurdes Inoue:DO NOT have relevant financial relationships
| Gillian Schmidler:No Answer
| Michael MacKenzie:DO NOT have relevant financial relationships
| Daniel Friedman:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Boston Scientific:Active (exists now)
; Research Funding (PI or named investigator):Phillips:Active (exists now)
; Consultant:MicroPort CRM:Past (completed)
; Consultant:Alleviant:Active (exists now)
; Consultant:Boston Scientific:Active (exists now)
; Consultant:Medtronic :Active (exists now)
; Consultant:Abbott:Active (exists now)
; Research Funding (PI or named investigator):Merit Medical:Past (completed)
; Research Funding (PI or named investigator):Medtronic:Active (exists now)
| William Abraham:No Answer
| John Cleland:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Pharmacosmos:Active (exists now)
; Individual Stocks/Stock Options:Viscardia:Active (exists now)
; Individual Stocks/Stock Options:Heartfelt:Active (exists now)
; Research Funding (PI or named investigator):CSL Vifor:Past (completed)
| Anne Curtis:DO have relevant financial relationships
;
Consultant:Medtronic:Active (exists now)
; Speaker:Sanofi Aventis:Active (exists now)
; Consultant:Janssen Pharmaceuticals:Active (exists now)
; Consultant:Abbott:Active (exists now)
; Speaker:Medtronic:Active (exists now)
| Michael Gold:DO have relevant financial relationships
;
Consultant:Boston Scientific:Active (exists now)
; Speaker:Abbott:Past (completed)
; Consultant:Medtronic:Past (completed)