Door-in to door-out time and in-hospital mortality in patients with ST-elevation myocardial infarction
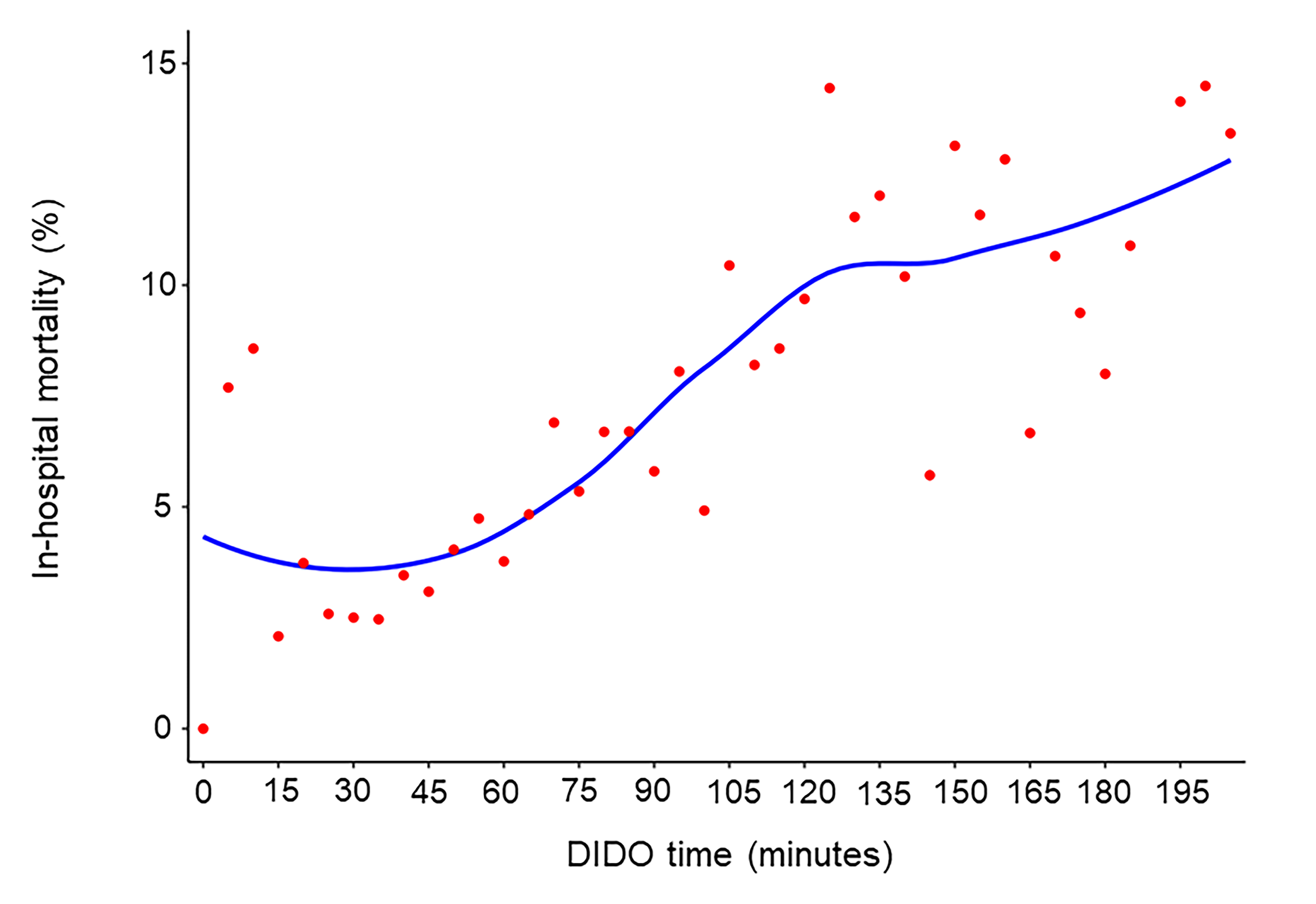
Abstract Body (Do not enter title and authors here): Background: Although current guidelines recommend achieving a door-in to door-out (DIDO) time within 30 minutes for 75% of patients with ST-elevation myocardial infarction (STEMI) who require interhospital transfer for primary percutaneous coronary intervention (PCI), disparities between guidelines and clinical performance persist. Methods: We analyzed the association between the DIDO time and in-hospital mortality using data from the Get With The Guidelines® – Coronary Artery Disease STEMI and NSTEMI Registry covering 232,935 admissions between the fourth quarter of 2019 and the third quarter of 2022. We determined the cut-off value of the DIDO time at which the odds of in-hospital mortality markedly increased by a likelihood ratio (LR) and an area under the curve (AUC) derived by generalized linear regression. Results: Of the 103,838 patients with STEMI, 23,865 (23%) required interhospital transfer. The median DIDO time was 63 (interquartile range 43–105) minutes and was within 30 minutes in 9% of cases. Generalized linear mixed models showed that a DIDO time delay of 5 minutes was significantly associated with higher in-hospital mortality (adjusted odds ratio [OR], 1.88; 95% confidence interval [CI], 1.56–2.27; p<0.001). The LR test and AUC showed that DIDO time cut-offs at 30, 42, 63, and 93 minutes were associated with increased in-hospital mortality. Compared with a reference DIDO time of within 30 minutes, the in-hospital mortality did not significantly differ for a DIDO time from 30 to 42 minutes (adjusted OR, 1.20; 95% CI, 0.83–1.73; p=0.340), but it was significantly higher for DIDO times from 42 to 63 minutes (adjusted OR, 1.48; 95% CI, 1.06–2.06; p=0.020), 63 to 93 minutes (adjusted OR, 1.89; 95% CI, 1.36–2.63; p<0.001), and over 93 minutes (adjusted OR, 2.85; 95% CI, 2.08–3.90; p<0.001). Conclusion: A delayed DIDO time was significantly associated with higher in-hospital mortality, particularly beyond 42 minutes.
Nakashima, Takahiro
(
University of Michigan
, Ann Arbor , Michigan , United States )
Kiyoshige, Eri
(
NCVC
, Suita , Japan )
Ogata, Soshiro
(
NCVC
, Suita , Japan )
Cranford, James
(
University of Michigan
, Ann Arbor , Michigan , United States )
Ali, Murtuza
(
LOUISIANA STATE UNIV SCH MEDICINE
, New Orleans , Louisiana , United States )
Kindipan, Ingrid
(
Methodist Charlton Medical Center
, Dallas , Texas , United States )
Tamis-holland, Jacqueline
(
The Cleveland Clinic
, Cleveland , Ohio , United States )
Nishimura, Kunihiro
(
NATL CEREBRAL AND CV CTR JAPAN
, Suita , Japan )
Goyal, Abhinav
(
The Emory Clinic
, Atlanta , Georgia , United States )
Neumar, Robert
(
UNIV OF MICHIGAN HEALTH SYSTEM
, Ann Arbor , Michigan , United States )
Author Disclosures:
Takahiro Nakashima:DO NOT have relevant financial relationships
| Robert Neumar:No Answer
| Eri Kiyoshige:DO NOT have relevant financial relationships
| Soshiro Ogata:DO NOT have relevant financial relationships
| James Cranford:DO NOT have relevant financial relationships
| Murtuza Ali:DO NOT have relevant financial relationships
| Ingrid Kindipan:DO NOT have relevant financial relationships
| Jacqueline Tamis-Holland:DO NOT have relevant financial relationships
| Kunihiro Nishimura:No Answer
| Abhinav Goyal:DO NOT have relevant financial relationships